Feline Pulmonary Langerhans Cell Histiocytosis
Pulmonary LCH is a disease of aged cats (10 to 15 years), which causes progressive respiratory failure leading to euthanasia (Vet Pathol. 2008;45(6):816–824). The cats present with severe respiratory distress characterized by tachypnea, increased respiratory effort or open mouthed breathing. The symptoms can be acute or present for several months. Thoracic radiographs reveal a diffuse broncho-interstitial pattern of miliary to nodular opacities throughout all lung lobes (Fig. 1). The original report described pulmonary LCH in 3 cats. Since then, 4 additional cases have been encountered (Moore, PF – unpublished data). All have been diagnosed at necropsy. Pulmonary LCH occurs in humans, especially among smokers. It is believed to be a reactive disorder, which often resolves following cessation of smoking. Clonality studies have been associated with mixed results; some lesions harbor clonal expansions of LCs, but the majority of lesions have polyclonal LC proliferation. A neoplastic process was favored in feline pulmonary LCH based on the cytological characteristics of the LC infiltrate and the consistent extra-pulmonary lesions. However, molecular clonality studies were not conducted in support of that conclusion.
Morphologic features
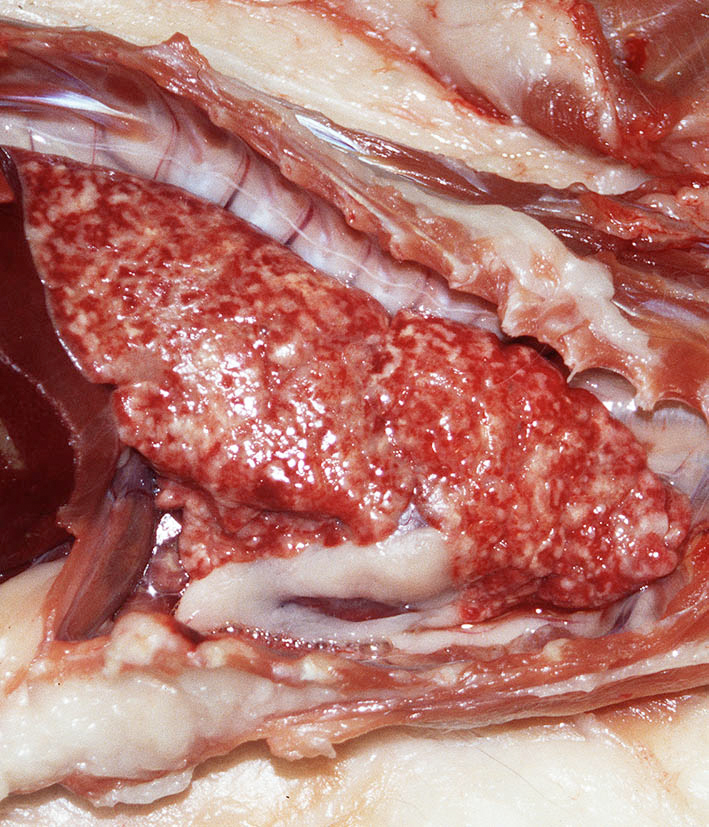
The macroscopic lesions are distinctive; an infiltrative process involves all lung lobes. The lungs are diffusely firm and entirely effaced by ill-defined, coalescing nodular masses (2 – 5 mm maximum dimension) (Fig. 2). These nodules often coalesced thereby effacing larger areas of parenchyma, which extended from peribronchiolar locations to the pleural surface. Extra-pulmonary spread to pancreas and kidney is variably observed. The tracheobronchial lymph nodes, and lymph nodes draining affected abdominal organs are also enlarged and diffusely effaced.
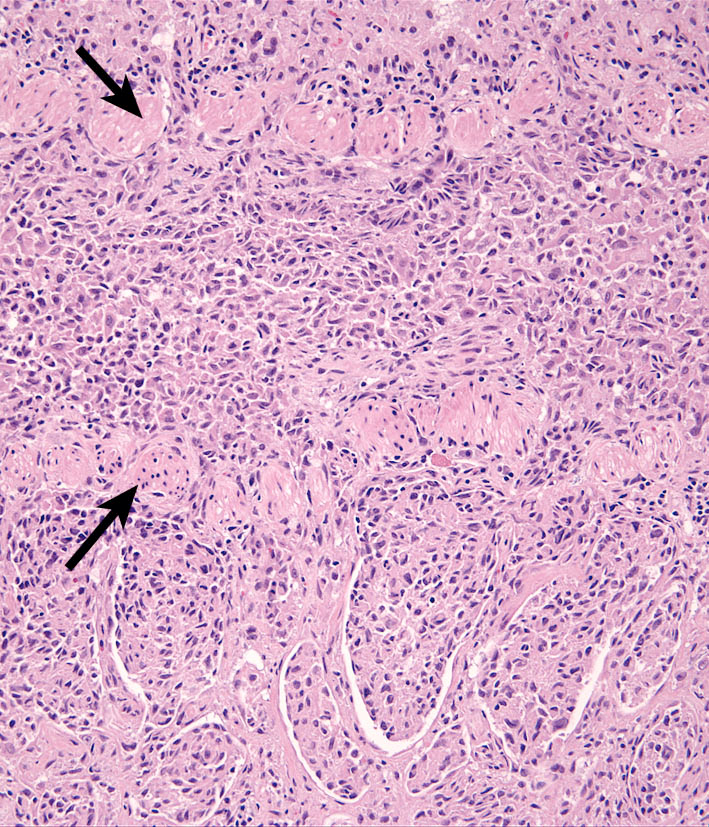
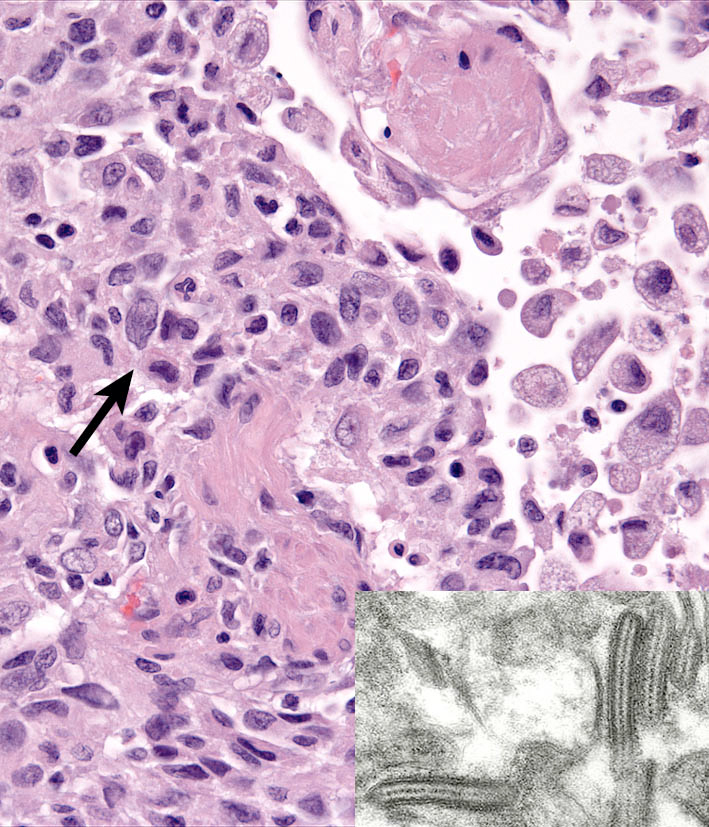
Pulmonary lesions are unique, and consist of histiocytic infiltrates within terminal and respiratory bronchioles. The infiltrates partially obliterate the airway walls and fill the lumens. Extension of the infiltrates into adjacent alveolar ducts and alveoli occurs (Fig. 3). Histiocytes form cohesive infiltrates with indistinct cell borders. They are moderately pleomorphic in cell size and nuclear morphology, which is often complex (convoluted, twisted or folded) (Fig. 4). Transmission electron microscopy was used to demonstrate characteristic BGs in the cytoplasm of lesional histiocytes; these structures are only present in LCs and their formation is dependent on the C-type lectin, langerin (Fig. 4 inset)

Immunophenotypic features
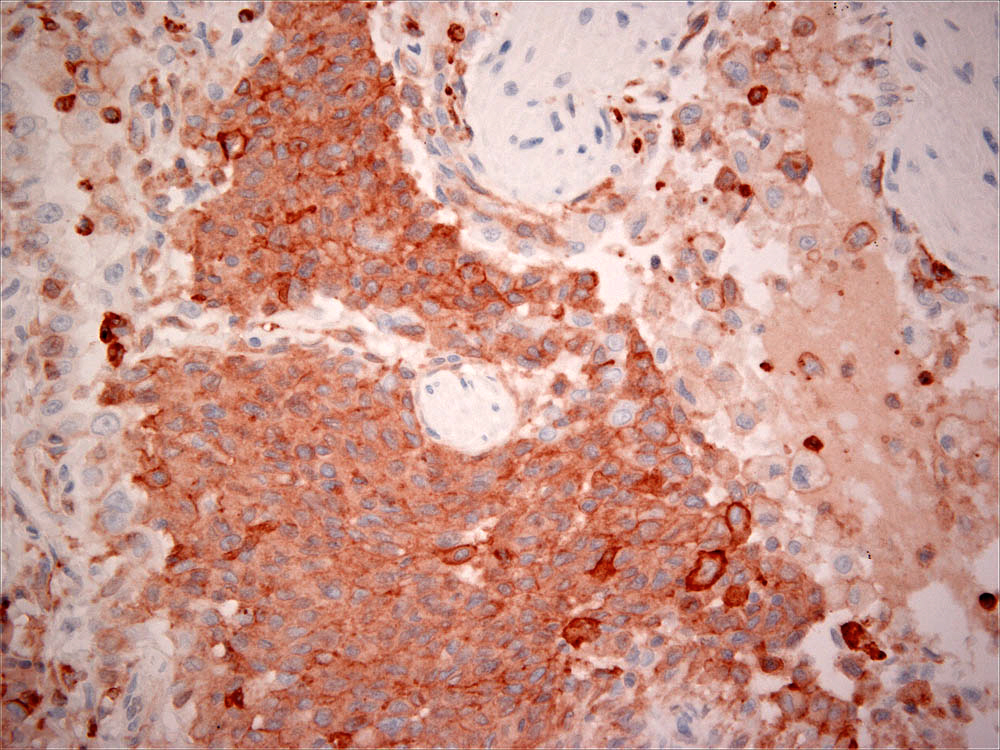
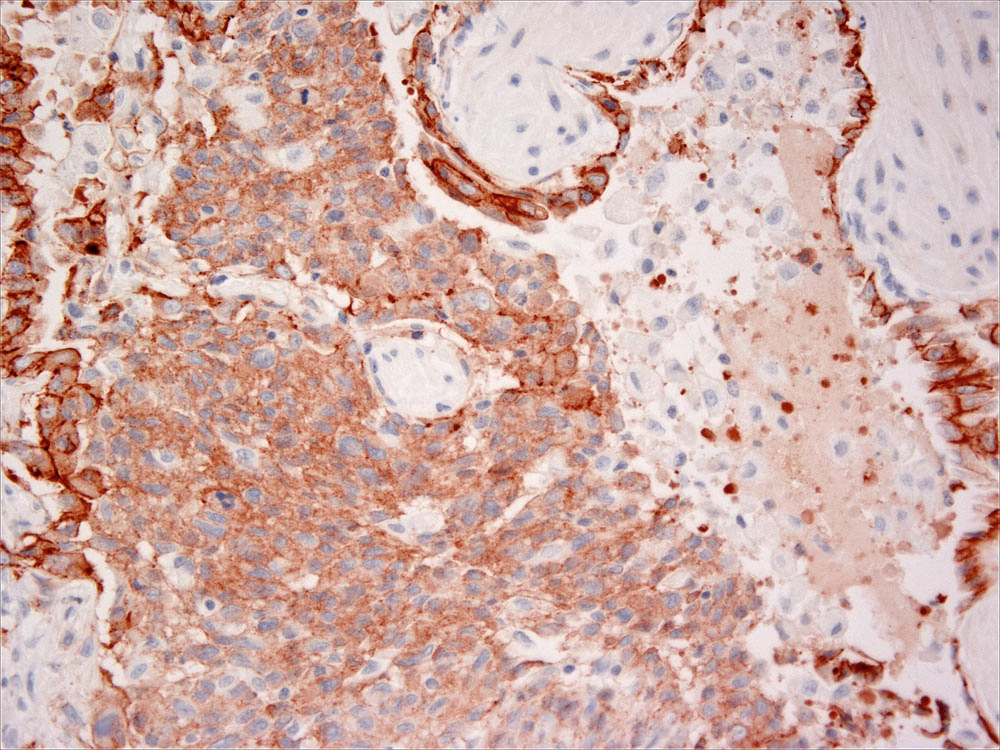
The lesional hisiocytes express CD18 (Fig. 5) and E-cadherin (Fig. 6). CD1 expression has not been evaluated in pulmonary LCH, as only formalin fixed tissues have been available. E-cadherin expression is most often markedly reduced in extra-pulmonary lesions. This may be indicative of active down-regulation of E-cadherin expression associated with LC migration; this occurs in normal LCs when they migrate from epithelia to lymph nodes.
-TOP-